What Is Apical Periodontitis?
Apical periodontitis, also called periapical periodontitis, begins when bacteria or inflammatory irritants from the pulp reach the periapical tissues around the root tip or apex. This means the infection inside the tooth triggers your body’s defence system, which then causes inflammation and irritation around the tip of the tooth root. It may be painful and obvious, or it may sit quietly in the bone and only appear as a dark shadow appearing at the tip of a tooth root on an X-ray. The condition is often missed until a dentist properly examines the tooth for that reason.
Deep decay, dental trauma, cracks, and sometimes operative dental procedures can damage the pulp enough to trigger this process. Bacteria may enter the tooth, triggering inflammation around the root tip. That inflammation can damage the tissues holding the tooth in place and lead to loss of bone around the end of the root. The infected or dying pulp, often after pulpal necrosis, is usually the main driver. The body’s immune response then causes inflammation and destruction in the periapical tissues around the root tip, including resorption of the surrounding alveolar bone.
The problem usually does not improve on its own if the bacteria remain trapped inside the tooth. The germs can stick to the inside of the root canals and hide in small spaces that the body cannot reach easily. Because of that, the infection can keep coming back or stay there. This is why treatment usually involves cleaning out the inside of the tooth with root canal treatment, repeating the treatment if needed, doing surgery in some cases, or removing the tooth if it cannot be saved.
Types of Apical Periodontitis
Apical periodontitis is commonly described as symptomatic or asymptomatic, and it may also be referred to as acute or chronic depending on how it presents.
- Symptomatic apical periodontitis often corresponds to acute apical periodontitis. Acute apical periodontitis typically causes pain with biting, tenderness to pressure or tapping, difficulty chewing in the area, and a sensation that the tooth is ‘high’ or slightly raised. At this stage, the inflammation may still be early enough that the X-ray shows little or no obvious change apart from a slight widening around the root tip.
- Asymptomatic apical periodontitis is often grouped with chronic apical periodontitis. In these cases, the tooth may not hurt at all, but the pulp is usually necrotic and infected, and the X-ray often shows a dark spot at the root tip, indicating bone involvement.
Apical Periodontitis Causes
The most common causes of apical periodontitis are untreated dental caries, trauma, cracks, exposed dentine or cementum, and pulp infection that progresses to necrosis.
Bacteria in the mouth can cause tooth decay and spread into the tiny channels inside the tooth. If the problem goes deeper, the nerve and soft tissue inside the tooth can become infected. Sometimes inflammation can also happen after irritation from dental chemicals, material pushed slightly beyond the root during treatment, or fillings and other materials placed inside the tooth. Because of this, apical periodontitis can happen in both untreated teeth and teeth that have already had dental treatment.
The condition develops because the body reacts to bacteria and bacterial by-products leaving the root canal system. At first, the inflammation can cause pain and tenderness around the tip of the tooth root. If the irritation stays there, the problem can become long-lasting. Even if the tooth stops hurting, unhealthy tissue can remain around the root tip, and the surrounding bone can slowly break down.
Symptoms
Symptoms of apical periodontitis range from no symptoms to marked pain, tenderness, swelling, and difficulty chewing.
In symptomatic apical periodontitis, patients often report pain on biting, soreness when the tooth is tapped, difficulty eating on that side, and a sensation of the tooth being raised. Some teeth are also sensitive to pressure or feel different from the surrounding teeth. If the infection worsens, swelling or a draining abscess may develop.
In chronic apical periodontitis, the tooth may cause no obvious discomfort and may be found only during routine radiographic evaluation. Sometimes there is no pain, even though the tissue around the root tip remains inflamed and the bone in that area is slowly being damaged. This is common in long-standing apical periodontitis, so a painless dark area around the root should not be assumed to be harmless.
When to See a Dentist
You should see a dentist if you have pain on biting, a tooth that feels raised, swelling of the gums, or a periapical radiolucency (dark spot) on an X-ray near the root tip.
A painful tooth that is tender when you bite, especially one with deep decay or a history of trauma, should be checked promptly. A review is also sensible if a previously treated tooth becomes uncomfortable again, or if a dentist has told you there is a periapical shadow on an X-ray, even though you do not feel symptoms. Early treatment can prevent the disease from worsening into abscess formation, fistula, or wider spread through the surrounding tissues.
A simple, practical rule for patients is this: if a tooth feels raised, is painful to bite on, or has nearby swelling, it is usually safer to get it examined sooner rather than later. Acute symptoms can escalate quickly, and chronic lesions can sit quietly while bone damage continues.
Diagnosis
Diagnosis of apical periodontitis depends on the clinical examination, pulp testing, symptom pattern, and dental imaging such as periapical radiography.
A dentist will usually begin by asking what the pain feels like, whether it is triggered by biting or temperature, how long it has been present, and whether the affected tooth has had previous treatment.
Testing pulp sensibility and vitality is important. In acute cases, the pulp may still be vital or may already be necrotic. The tooth is often sore when the dentist taps on it. Early on, the X-ray may still look normal or show only slight changes around the root. In long-standing cases, the nerve inside the tooth is usually dead and infected, so the tooth often does not respond to standard nerve tests. The X-ray is also more likely to show a dark area around the root tip, suggesting infection and bone damage.
The diagnosis also involves ruling out other causes of apical shadows and pain. Some periapical lesions that appear similar on X-ray can represent granulomas, cysts, or non-endodontic findings, so the dentist must interpret the radiograph alongside the clinical picture rather than relying on the image alone. Histological analysis of the removed tissue can confirm the nature of a lesion when needed.
Non-Surgical Management
Non-surgical management aims to remove the source of infection from inside the tooth and seal the root canal system to prevent reinfection.
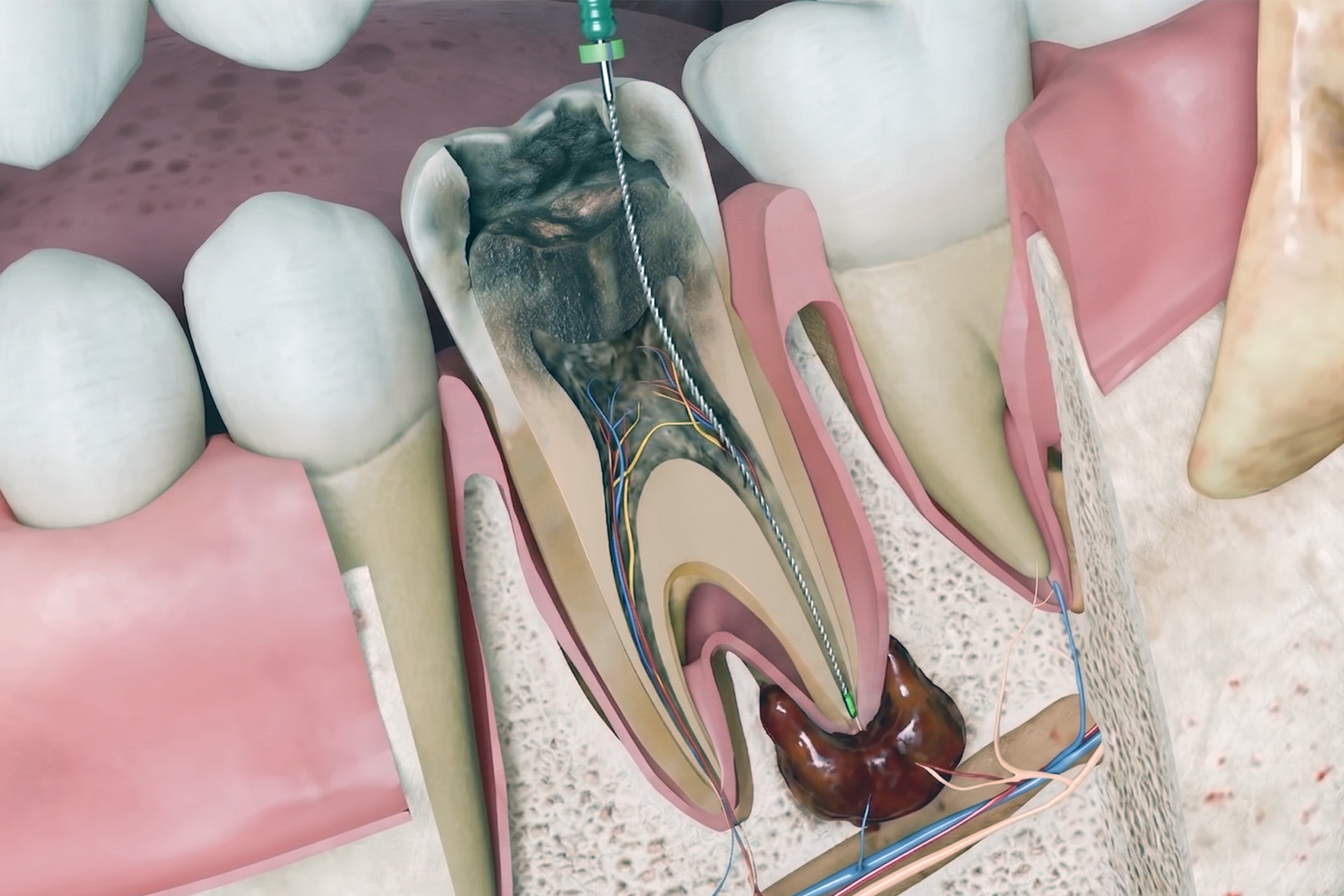
The usual treatment plan for apical periodontitis begins with nonsurgical endodontic treatment, usually root canal treatment, if the tooth is restorable and has not already been treated. The aim is to remove bacteria from the root canal, remove infected tissue and debris, avoid pushing cleaning fluids past the root tip, and then sealing the canal with a filling to help prevent the infection from returning. When root canal therapy is done well, the dark area around the root tip on the X-ray often shrinks over time as the area heals.
If the tooth has already had root canal treatment and the lesion persists or returns, it is called post-treatment apical periodontitis, or persistent apical periodontitis. Non-surgical endodontic retreatment may be needed when the infection persists due to missed canals, inadequate cleaning, poor access, restoration leakage, or difficult root canal anatomy. Root canal-treated teeth and other endodontically treated teeth that show new symptoms or an enlarging lesion are reviewed for endodontic failure, including late endodontic treatment failure due to persistent intraradicular infection or recurrent disease.
Antibiotics are not a routine treatment for apical periodontitis on their own. They are generally reserved for cases with rapid onset, fever, malaise, swollen lymph nodes, spreading infection, or immunocompromised patients. In most ordinary cases, the central issue is the infected root canal system, which must be treated by a dentist rather than with tablets alone.

Surgical Options
Surgical treatment is considered when non-surgical endodontic care is unlikely to solve the problem or when disease persists after treatment.
If the apical disease persists despite the appropriate root canal or endodontic retreatment, periapical surgery may be an option to save the tooth. Apical surgery, also called endodontic surgery or endodontic microsurgery, often takes the form of an apicoectomy, in which the infected periapical tissues around the root tip are removed, the end of the root is resected, and a root-end filling is placed.
Extraction remains an option when the tooth cannot be predictably restored or retained, such as in cases of severe structural damage, poor restorative prognosis, or when endodontic treatment is not sensible. Prolonged infection can even cause resorption of the external apical root surface. The aim is always to preserve the natural tooth where possible, but not at the expense of prolonged infection or poor long-term outcomes.
Risks and Recovery
Untreated apical periodontitis can progress to abscess formation, fistula and bone destruction, while recovery after treatment is usually gradual and radiographic.
If the infection is not treated, a sudden, painful problem can worsen, and a long-standing infection can continue damaging the tissue around the tip of the root without causing obvious symptoms. The area may fill with unhealthy healing tissue, and in some cases, the infection can spread through to the bone, form a small channel that drains pus into the mouth, or turn into an abscess. The bone around the root can also continue to break down over time. Even if there is no pain, this kind of hidden infection still matters because it can continue to harm the tooth and surrounding tissues, and an ongoing dental infection may also affect overall health.
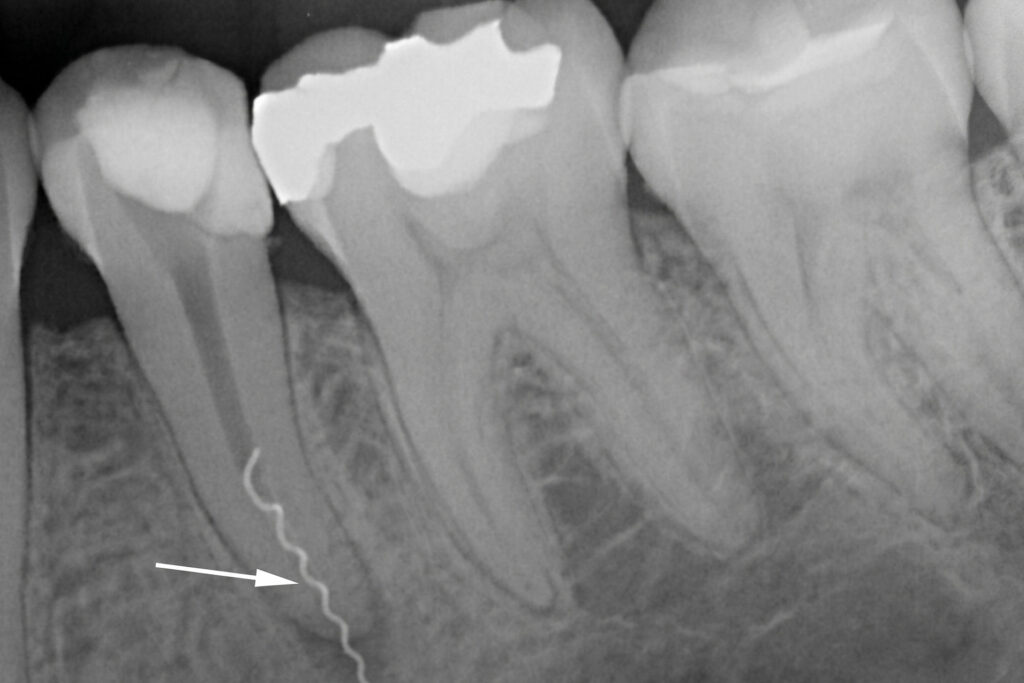
Healing after treatment is usually monitored over time rather than judged in a few days. Many periapical lesions improve within six months to two years, and the follow-up periapical radiography helps show whether the periapical radiolucency is shrinking as expected. Further management is usually considered if the periapical radiolucency remains unchanged after about a year, increases in size, or appears in a previously endodontically treated tooth without prior apical disease. A lesion in a treated tooth without prior apical disease will suggest new infection; if a periapical radiolucency remains unchanged or enlarges, retreatment will be considered.
Some patients experience a short-term flare-up with pain or swelling after endodontic treatment. This can happen within hours or days and does not always mean the treatment has failed. However, it does need proper review if the symptoms are significant or worsening.
How TEETH @ Tiong Bahru Can Help
TEETH @ Tiong Bahru can help by identifying whether the problem is active apical disease, clarifying whether the affected tooth is still restorable, and planning the right endodontic care for you.
This starts with a careful examination, appropriate pulp testing, and radiographs that help interpret both the symptoms and the images. Some teeth need primary root canal treatment. Some need nonsurgical endodontic retreatment. Others need surgical referral, such as periapical surgery. And some are better managed by extraction when the tooth structure is too compromised.
The long-term success of apical periodontitis treatment also depends on what happens after the root canal itself. A sound final restoration, good oral hygiene, and follow-up reviews all help reduce the risk of reinfection and persistent inflammation in root-filled teeth. When apical periodontitis is caught early and managed properly, many teeth can be kept comfortable and functional for years.
Schedule your consultation with our dentists at TEETH @ Tiong Bahru today.





